
 Discussion
Discussion
Ultomiris for paroxysmal nocturnal hemoglobinuria
Last updated Nov. 4, 2025, by Margarida Maia, PhD
 Fact-checked by Lindsey Shapiro, PhD
Fact-checked by Lindsey Shapiro, PhD
What is Ultomiris for PNH?
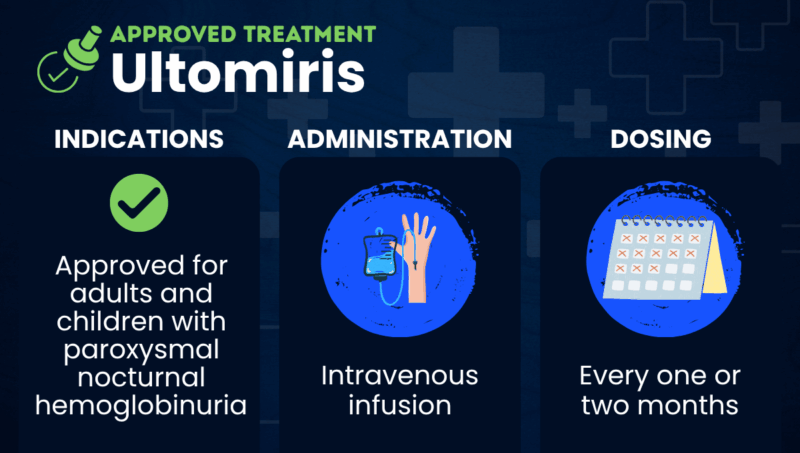
Ultomiris (ravulizumab-cwvz) is a complement inhibitor that’s approved to treat adults and children with paroxysmal nocturnal hemoglobinuria (PNH). It is delivered by intravenous (into-the-vein) infusion.
In PNH, red blood cells are lacking proteins on their surface that normally tell the immune system that the cells are a healthy part of the body and shouldn’t be attacked. Without these proteins, a part of the immune system called the complement system attacks and destroys red blood cells, which is known as hemolysis.
Ultomiris is designed to block the activation of a complement protein called C5, thereby preventing it from triggering hemolysis and, in turn, easing the symptoms of PNH.
The therapy was developed by Alexion Pharmaceuticals, now part of AstraZeneca, and is also approved for treating other complement-mediated disorders. Ultomiris works similarly to the company’s other approved complement inhibitor, Soliris (eculizumab), but is designed to last longer in the body. This means it requires about four times fewer infusions than Soliris, which may ease the treatment burden for people with PNH.
Therapy Snapshot
Scroll horizontally to view all columns -->
| Brand Name: | Ultomiris |
| Chemical Name: | Ravulizumab-cwvz |
| Usage: | Used to prevent hemolysis and ease symptoms in PNH |
| Administration: | Intravenous infusion |
Who with PNH can take Ultomiris?
Ultomiris is approved in the U.S. to treat adults and children, ages 1 month and older, with PNH. It is similarly approved in other countries, although the specific indication may vary. In the European Union, it can be used to treat adults and children who weigh at least 10 kg (22 pounds).
In the U.S., Ultomiris is available only through a restricted access program because it increases the risk of serious and life-threatening meningococcal infections, for which it carries a boxed warning.
The treatment should not be used in any patient with an unresolved, serious infection with Neisseria meningitidis, the bacteria that causes meningococcal disease.
How is Ultomiris administered in PNH?
Ultomiris is administered via intravenous infusion by a medical professional in an infusion clinic, at a healthcare provider’s office, or, in some cases, at a patient’s home. The duration varies, but infusions typically last less than an hour for most adults. Patients are monitored for infusion reactions for at least one hour afterward.
Starting two weeks after an initial loading dose, Ultomiris is infused every eight weeks for most patients — resulting in six or seven infusions per year — and every four weeks for children weighing less than 20 kg (44 pounds). Dosing also varies according to body weight, with loading doses ranging from 600 to 3,000 mg, and maintenance doses ranging from 300 to 3,600 mg.
Ultomiris in PNH clinical trials
Ultomiris’ approval for PNH was backed by data from three Phase 3 clinical trials. In those trials, the medication was shown to be as effective as Soliris for controlling hemolysis and enabling PNH patients to remain free of blood transfusions.
- In ALXN1210-PNH-301 (NCT02946463), 246 adults with PNH who had not been previously treated with a complement inhibitor were given either Ultomiris or Soliris. After six months, at least two-thirds of patients on either therapy were free of blood transfusions (73.6% vs. 66.1%). About half had reached normal levels of lactate dehydrogenase (LDH), a marker of hemolysis (53.6% vs. 49.4%).
- In ALXN1210-PNH-302 (NCT03056040), 195 adults who were clinically stable after being on Soliris for at least six months were randomly assigned to either continue treatment with Soliris or switch to Ultomiris. After six months, most patients in the two groups remained free of blood transfusions (87.6% vs. 82.7%), with changes in LDH levels also being identical.
- In ALXN1210-PNH-304 (NCT03406507), 13 children and adolescents with PNH received open-label treatment with Ultomiris. Some had previously received Soliris. None of the participants, who ranged in age from 9 to 17, experienced breakthrough hemolysis, and most (84.6%) avoided blood transfusions. Reductions in LDH were consistent with those observed in adults.
Ultomiris side effects
The most common side effects associated with Ultomiris in PNH patients include:
- upper respiratory tract infection
- headache
Per the boxed warning, Ultomiris increases the risk of serious meningococcal infections caused by N. meningitidis. As such:
- Patients should complete or update their meningococcal vaccines at least two weeks before starting Ultomiris. If treatment must begin right away and vaccination is incomplete, patients should receive the required vaccines as soon as possible. They may also need antibiotics.
- All individuals on Ultomiris should be monitored closely for signs and symptoms of meningococcal infections, as these can quickly become life-threatening if not recognized and treated early.
People on Ultomiris may also be at an increased risk of other types of infections.
Some patients receiving Ultomiris may have infusion-related reactions, including serious allergic reactions (anaphylaxis) and hypersensitivity. Patients will be closely monitored for such reactions, and the infusion should be stopped if heart or lung problems occur.
After discontinuing Ultomiris, patients should also be closely monitored for the return of signs and symptoms of hemolysis.
PNH News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
FAQs about Ultomiris
Category:
Ultomiris
There is no known interaction between alcohol and Ultomiris. However, because alcohol can affect some treatments, patients should talk with their healthcare team before drinking alcohol while on Ultomiris.
Category:
Ultomiris
There is no information on the use of Ultomiris during pregnancy in humans, however, in animal studies, a similar medication caused harm to the developing fetus. That risk must be weighed with the fact that pregnancy in women with untreated paroxysmal nocturnal hemoglobinuria carries a higher risk of complications for both mother and baby. Patients who are pregnant or planning to become pregnant should talk with their healthcare team.
Category:
Ultomiris
Hair loss and weight gain have not been reported as side effects of Ultomiris in people with paroxysmal nocturnal hemoglobinuria. Patients should talk with their healthcare team if they experience any unexpected side effects.
Category:
Ultomiris
In clinical trials, some people with paroxysmal nocturnal hemoglobinuria who were treated with Ultomiris started to see reductions in biomarkers of red blood cell destruction (hemolysis) within two weeks. However, results may vary, so patients should talk with their healthcare team about how Ultomiris may help in their particular case.
Category:
Ultomiris
The U.S. Food and Drug Administration approved Ultomiris for adults with paroxysmal nocturnal hemoglobinuria in 2018 and for children, ages 1 month and older, in 2021. Ultomiris is also approved in the U.S. for atypical hemolytic uremic syndrome, generalized myasthenia gravis, and neuromyelitis optica spectrum disorder.
Related Articles
-
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
Discussion
-
 Discussion
Discussion
-
Discussion