
 Fact-checked by
Fact-checked by  Discussion
Discussion
Fabhalta (iptacopan) for paroxysmal nocturnal hemoglobinuria
What is Fabhalta for PNH?
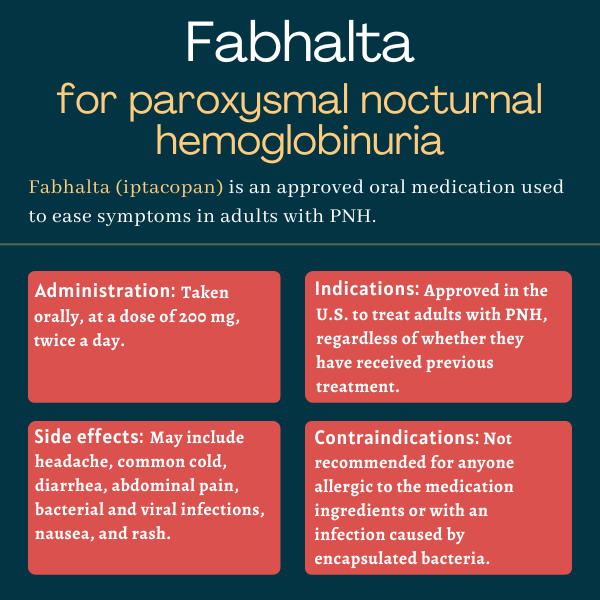
Fabhalta (iptacopan) is an oral therapy approved in the U.S. for adults with paroxysmal nocturnal hemoglobinuria (PNH), including those previously treated and those who have not received any prior treatment.
Developed by Novartis, Fabhalta is designed to ease disease symptoms and is the first single oral therapy available for PNH.
The therapy also is being developed as a potential treatment for diseases other than PNH that are associated with overactivation of the immune complement system, a part of the immune system that helps the body fight off infections. These include: atypical hemolytic uremic syndrome, immunoglobulin A nephropathy, C3 glomerulopathy, and immune complex membranoproliferative glomerulonephritis.
Therapy snapshot
Scroll horizontally to view all columns -->
| Brand name: | Fabhalta |
| Chemical name: | Iptacopan |
| Usage: | Treatment of adults with paroxysmal nocturnal hemoglobinuria |
| Administration: | Oral capsules |
How does Fabhalta work?
PNH is a rare disease mostly caused by mutations that lead to the complete or partial loss of two proteins in blood cells that work as identification badges that let the immune system know these are a healthy part of the body.
These proteins particularly suppress the complement cascade, a set of immune proteins in circulation that are activated in a domino-like way, with the activation of one protein leading to the activation of the next and so on.
Without the identification badges, healthy blood cells, including red blood cells, become susceptible to complement-mediated destruction. As such, PNH is characterized by red blood cell breakdown (hemolysis), leading to symptoms of anemia, or deficient levels of hemoglobin in red blood cells. Hemoglobin is the protein that carries oxygen throughout the body.
In PNH, red blood cell destruction occurs both inside blood vessels (intravascular hemolysis) and outside blood vessels, mostly in the liver and spleen (extravascular hemolysis).
Intravascular hemolysis depends on the cleavage of the complement component 5 (C5) — the target of two other approved PNH therapies, Soliris (eculizumab) and Ultomiris (ravulizumab) — while extravascular hemolysis is facilitated by C3, a protein positioned earlier than C5 in the complement cascade.
A first-in-class medication, Fabhalta works by suppressing factor B, a protein of the complement system that is involved in C3 activation, which ultimately leads to the cleavage of C5.
By suppressing complement activation at an early point in the cascade, Fabhalta is expected to prevent both intravascular and extravascular hemolysis, consequently helping to restore red blood cell and hemoglobin levels and easing PNH symptoms.
Who can take Fabhalta?
Fabhalta was approved by the U.S. Food and Drug Administration (FDA) in December 2023 for the treatment of adults with PNH, regardless of whether they had received any prior treatment.
The decision made Fabhalta the first oral monotherapy, or single therapy, approved for this rare disease, and the only FDA-approved treatment targeting factor B.
Because the therapy can increase the risk of potentially life-threatening infections caused by encapsulated bacteria, the medication is available in the U.S. only through a restricted access program.
Called Fabhalta REMS — REMS stands for Risk Evaluation and Mitigation Strategy — the program ensures only certified healthcare professionals can prescribe Fabhalta, that both physicians and patients are informed about this potential risk, and vaccination against these encapsulated bacteria is up to date in all patients before Fabhalta treatment initiation.
Who should not take Fabhalta?
Fabhalta is not recommended for anyone with:
- a known serious allergy to the medication or any of its ingredients
- a serious and unresolved infection caused by encapsulated bacteria, including Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae type B.
The therapy also should not be taken by anyone with severe kidney or liver problems. It is not recommended for patients taking medications that are strong suppressors of CYP2C8, a liver enzyme that is involved in the metabolism of several medications.
Fabhalta’s prescribing label has a boxed warning for serious, life-threatening infections with encapsulated bacteria, as these have occurred in vaccinated and unvaccinated patients treated with complement inhibitors.
For this reason, patients initiating the therapy should complete or update their vaccination against encapsulated bacteria, unless the risks of delaying Fabhalta treatment outweigh the risks of developing a potentially serious infection. They also should be closely monitored for signs of infection.
How is Fabhalta administered?
Fabhalta is available in opaque, pale yellow, hard gelatin capsules containing 200 mg of the medication. Each capsule is imprinted with LNP200 on the body and NVR on the cap.
The recommended dose is a 200 mg capsule twice a day, with or without food. Capsules should be swallowed whole, and should not be opened, broken, or chewed.
If a planned dose is missed, patients should take a Fabhalta capsule as soon as possible, even if it’s almost time for the next scheduled dose, and then resume the regular dosing scheme.
Given that medications promoting activity of the CYP2C8 enzyme, such as the antibiotic rifampin, may reduce Fabhalta exposure, and therefore its efficacy, clinical response should be closely monitored in patients taking both Fabhalta and CYP2C8 inducers. If there are signs of loss of Fabhalta efficacy, the CYP2C8-inducing medication should be discontinued.
For patients switching from other specific PNH therapies, Fabhalta should be initiated no later than one week after the last dose of Soliris, or six weeks following the last dose of Ultomiris.
Fabhalta in clinical trials
The approval of Fabhalta was mainly supported by positive data from two multinational Phase 3 clinical trials: APPLY-PNH (NCT04558918) and APPOINT-PNH (NCT04820530). Both evaluated the safety and efficacy of the now-approved dose of 200 mg of Fabhalta, taken twice daily, in adults with PNH.
APPLY-PNH
The APPLY-PNH study enrolled 97 patients at sites in the U.S., Brazil, and countries in Europe and Asia. All were experiencing residual anemia despite being on standard anti-C5 treatment (Soliris or Ultomiris) for at least six months.
Participants were randomly assigned to either initiate Fabhalta treatment (65 patients) or continue their stable standard treatment (32 patients) for about six months. Both Soliris and Ultomiris are administered directly into the bloodstream.
The trial’s main goals were to assess the proportion of patients experiencing a sustained, clinically meaningful increase of 2 g/dL or more in their hemoglobin levels and the proportion of those showing sustained hemoglobin levels of 12 g/dL (near-normal) or higher, both in the absence of blood transfusions.
Results showed Fabhalta significantly outperformed standard care at increasing hemoglobin levels, meeting both main goals of the study. Specifically, most Fabhalta-treated patients (82.3%) achieved a hemoglobin increase of at least 2 g/dL without the need for blood transfusions compared with none in the standard of care group.
Also, about two-thirds (67.7%) of patients on Fabhalta achieved at least near-normal hemoglobin levels without transfusions versus none of those continuing on standard anti-C5 treatment. Nearly all Fabhalta-treated patients (95.2%) also avoided blood transfusions altogether, compared with 45.7% of those in the standard care group.
Patients completing the six-month treatment period could enter the trial’s extension phase, in which all received Fabhalta for about six months.
Final one-year results demonstrated continuous Fabhalta treatment maintained near-normal hemoglobin levels (mean of 12.2 g/dL), with 91.9% of patients remaining free of blood transfusions in the last six months of treatment. Longer treatment also was associated with reductions in patient-reported fatigue, as assessed with the Functional Assessment of Chronic Illness Therapy – Fatigue score.
Similar benefits were observed for participants switching from standard treatment to Fabhalta in the extension period. After six months on Fabhalta, mean hemoglobin levels were increased to near-normal (from 9.1 to 12.1 g/dL), 94.1% of these patients had avoided blood transfusions, and fatigue also was lessened.
There were no new safety concerns with longer treatment.
APPOINT-PNH
The APPOINT-PNH trial, conducted at European and Asian sites, enrolled 40 patients who had not previously received therapies that suppress the complement system. All had low hemoglobin levels and excessive levels of a hemolysis marker called lactate dehydrogenase (LDH).
All participants were treated with Fabhalta for six months, and results showed 77.5% of them achieved a sustained hemoglobin increase of at least 2 g/dL in the absence of blood transfusions, meeting the trial’s main goal.
A sensitivity analysis that included hemoglobin test results from local labs when central labs were not available found an even higher percentage of patients — 87.5% — achieved this goal.
Data presented at a scientific meeting also indicated that most patients remained free from transfusions. Fabhalta treatment was associated with a reduction in LDH levels and patient-reported fatigue.
Ongoing trials
Those completing APPLY-PNH or APPOINT-PNH could enroll in an ongoing open-label extension study (NCT04747613) that’s assessing Fabhalta’s safety and efficacy for up to five years of treatment. The trial, which also included patients who participated in Fabhalta Phase 2 trials, is expected to end in 2027.
A multinational Phase 3 trial, called APPULSE (NCT05630001), is testing Fabhalta in up to 50 adults with PNH who were responding to stable treatment with either Soliris or Ultomiris (that is, with mean hemoglobin level of 10 g/dL or higher). Participants will switch from their standard treatment to Fabhalta for about six months.
The trial’s main goal is to evaluate whether the Novartis therapy is not inferior to standard anti-C5 treatment at preventing a reduction in hemoglobin levels. Secondary goals include hemoglobin changes suggestive of Fabhalta’s potential superiority; the proportion of patients showing blood-based response to the therapy; and changes in LDH levels, fatigue, and treatment satisfaction.
APPULSE is set to be completed in 2025.
Common side effects of Fabhalta
The most common side effects of Fabhalta in clinical trials include:
- headache
- common cold
- diarrhea
- abdominal pain
- bacterial infection
- viral infection
- nausea
- rash.
Serious infections caused by encapsulated bacteria
Fabhalta carries a boxed warning for an increased risk of serious encapsulated bacterial infections while on the therapy. These infections — which have been reported in both vaccinated and unvaccinated patients treated with complement inhibitors — can rapidly become life-threatening or fatal if not detected and treated early.
Patients starting on Fabhalta should be vaccinated against encapsulated bacteria according to current guidelines for those on complement inhibitors; all should complete or update the vaccination at least two weeks before initiating treatment.
If the risks of delaying treatment outweigh the potential risks of encapsulated bacterial infections, a patient who is not up to date with such vaccines may start Fabhalta, as long as they start preventive antibacterial treatment and receive the vaccines as soon as possible.
Given that vaccines against these bacteria reduce but do not completely eliminate the risk of infection, patients on Fabhalta should be routinely monitored for early signs of serious infections. These may include fever with or without shivers or chills, with either chest pain and cough, high heart rate, headache, or a rash, as well as headache with nausea or vomiting, body aches with flu-like symptoms, and sensitivity to light.
In the presence of signs or symptoms of a serious infection, patients should immediately seek medical care and infections should be promptly treated.
Because Fabhalta works by reducing immune activity and may affect the body’s ability to fight infections, its interruption may be considered for patients who are undergoing treatment for serious infections.
High levels of fatty molecules
Fabhalta may increase the blood levels of fatty molecules, including total cholesterol, low-density lipoprotein cholesterol (sometimes called bad cholesterol), and triglycerides.
In clinical trials, at least about one-quarter of patients with normal cholesterol and triglycerides levels at study’s start experienced an increase with Fabhalta that surpassed the normal level range. Some of these patients needed treatment with cholesterol-lowering medications.
Blood levels of these fatty molecules should be monitored regularly during Fabhalta treatment, and cholesterol-lowering medication should be initiated if necessary.
Patient monitoring after Fabhalta discontinuation
Patients stopping Fabhalta treatment should be closely monitored for at least two weeks after discontinuation for signs and symptoms of hemolysis, including blood in urine, fatigue, shortness of breath, and major cardiovascular events.
If such signs are detected, physicians should consider Fabhalta reinitiation, if appropriate, or the start of another PNH therapy.
Use in pregnancy and breastfeeding
There are limited trial data regarding Fabhalta’ effects on pregnancy outcomes, but studies in pregnant rats and rabbits suggested the therapy does not cause harm to the fetus.
Given that PNH, if left untreated, poses risks to the mother and fetus, patients who are pregnant or planning to become pregnant should discuss with their healthcare team the potential benefits and risks of using Fabhalta in these circumstances.
It is not known if Fabhalta can be found in breast milk and whether it has any impact on nursing infants or on milk production. But because many medications pass into human breast milk and can potentially cause serious adverse reactions in a nursing child, it is recommended breastfeeding be stopped during Fabhalta treatment and for five days after the last dose.
PNH News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
Discussion
-
 Discussion
Discussion
-
Discussion